Diastasis recti abdominis, pelvic floor and the abdominals.
 The post-natal period is often a hard time for women both physically and mentally. Today we’ll have a look at diastasis recti abdominis and why lower abdominal strength and the pelvic floor plays such an important role in women’s recovery from childbirth.
The post-natal period is often a hard time for women both physically and mentally. Today we’ll have a look at diastasis recti abdominis and why lower abdominal strength and the pelvic floor plays such an important role in women’s recovery from childbirth.
The postpartum period is often defined as six to eight weeks from delivery, but many physical changes are identified up to 12 months and years after delivery. Many changes occur during the post-partum period, expansion of the abdominal wall to accommodate the growing foetus during pregnancy commonly leaves prominent persistent physiological changes.
So, what is diastasis recti abdominis?
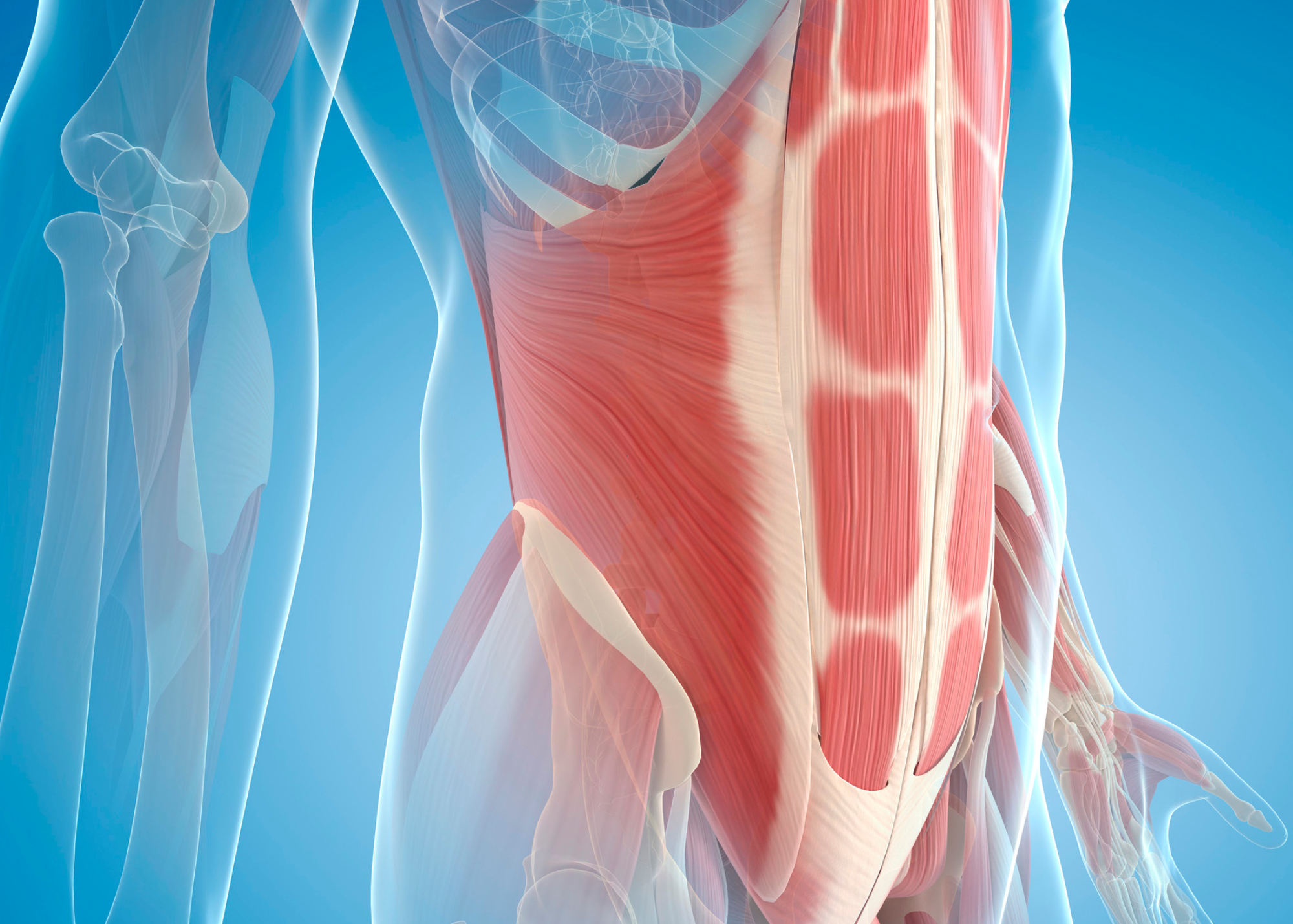 Diastasis recti abdominis is more commonly referred to as abdominal separation or DRAMS. It is defined as the separation of the two muscle bellies of rectus abdominis that results in abdominal bulging, believed to be associated with weakening of the linea alba (line running down the middle of your abdominals) either above the umbilicus, below the umbilicus or both. The linea alba is made of collagen fibres from both sides of the abdominal wall running from the xiphoid process to the symphysis pubis in an interwoven pattern that ensures core stability under abdominal muscle tension and accommodates intra abdominal volume. This weakens through multiple pregnancies as the rectus abdominis muscle elongates around the abdomen to accommodate the growing foetus.
Diastasis recti abdominis is more commonly referred to as abdominal separation or DRAMS. It is defined as the separation of the two muscle bellies of rectus abdominis that results in abdominal bulging, believed to be associated with weakening of the linea alba (line running down the middle of your abdominals) either above the umbilicus, below the umbilicus or both. The linea alba is made of collagen fibres from both sides of the abdominal wall running from the xiphoid process to the symphysis pubis in an interwoven pattern that ensures core stability under abdominal muscle tension and accommodates intra abdominal volume. This weakens through multiple pregnancies as the rectus abdominis muscle elongates around the abdomen to accommodate the growing foetus.
DRAMS is measured by touching 4.5cm above and below the umbilicus using an abdominal crunch in supine; women are classified into four categories dependant on number of finger breadths.
How common is it?
The prevalence of DRAMS in 12 months post-partum population is 32.6%. Despite this prevalence, the exact aetiology and risk factors are still under high debate.
Risk factors can include high age of mother, multi-parity, caesarean section particularly in those who have had multiple children and weight gain or obesity; as these elevate intra abdominal pressure or from abdominal surgery. It can occur in both men and women, although pregnancy is the most common cause, thought to be due to the increase in intra abdominal pressure from the growing foetus and hormonal changes. There is a higher likelihood of DRAMS among post-natal women who are exposed to heavy lifting 20 times a week or more.
What can you do if you think you may have DRAMS?
Firstly, all women should see a pelvic floor specialist or pelvic floor physio post childbirth for a proper pelvic floor assessment, as some women will have an overactive pelvic floor while others will have weakened muscle in need of more support. Multidisciplinary care can really help women move forward, here at Myothrive we work with women health physios regularly and communicate for the best outcome for our patients!
From here you will be given a unique program to start working your pelvic floor, any muscle weakness you may have through your abdominal area and hips, it may also include a balance activity. Everyone is unique with the timing and exercises they require, it’s not a cookie cutter plan.
Here some things we would look at implementing.
- Diaphragmatic breathing exercises should first involve focused belly breathing contracting the abdominals on exhale as a foundation, progressing to more specific mindful focus on the area of diastasis, breathing through isometric abdominal contractions then integrating the pelvic floor muscles.
- Exercises targeting transverse abdominis in conjunction with all the abdominal muscles, and pelvic floor muscles to help decrease intra-abdominal pressure and laxity of the linea alba to assist in more effective load transfer across the midline.
- Restoring strength and function. Strength exercises can include glute bridges progressing to marches, dead bugs variations, bird dog then modified plank variations.
What is the link between DRAMS and the pelvic floor?
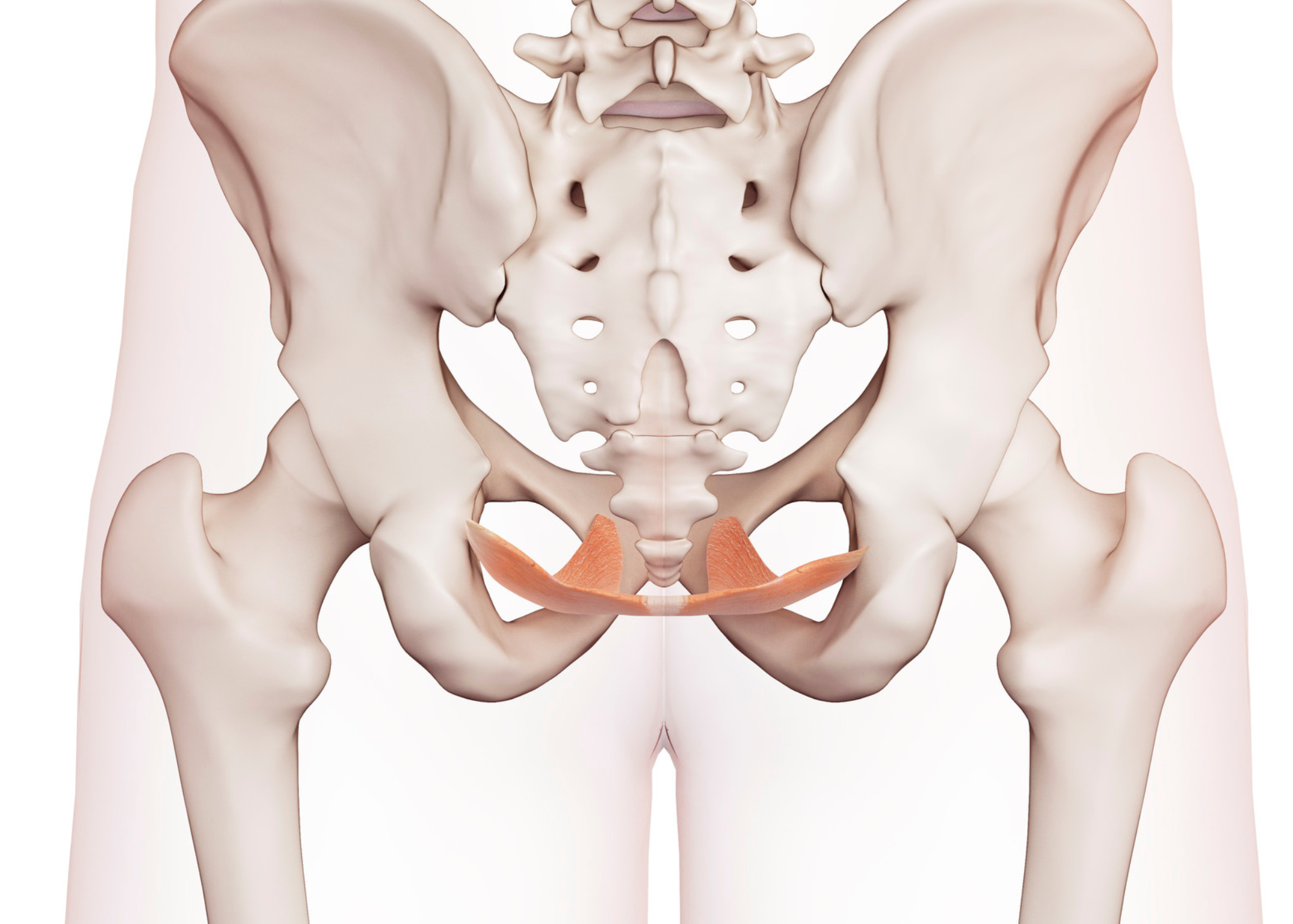 Breathing plays a large role in the interaction between pelvic floor, abdominals and diaphragm; this will also have an effect on continence and respiration. Contraction and relaxation of the diaphragm is affected by the contraction of the abdominals which if occurring simultaneously increases intra-abdominal pressure, thus trunk stability can be increased with simultaneous contraction of the diaphragm and abdominals. The pelvic floor does not independently contract itself but reacts and controls changes in intra-abdominal pressure by working with the diaphragm and abdominals, relaxing briefly on inspiration to allows downward movement of the diaphragm then co contracting with the abdominals during exhalation and coughing allowing upward movement of the diaphragm by increase IAP. Thus, providing active support through constant contraction while passive support of the pelvic occurs through form closure of the sacroiliac joint or SIJ. Force closure of the pelvis refers to interlocking of the joint surfaces, whereas form closure is through compressive forces of the muscles, ligaments, fascia and provides passive stability. Therefore, patients with DRAMS and a weakened linea alba, have poor form closure when performing a curl up task highlighting reduced IAP, reduced trunk mechanics and pelvic instability due to the lack of muscular passive support.
Breathing plays a large role in the interaction between pelvic floor, abdominals and diaphragm; this will also have an effect on continence and respiration. Contraction and relaxation of the diaphragm is affected by the contraction of the abdominals which if occurring simultaneously increases intra-abdominal pressure, thus trunk stability can be increased with simultaneous contraction of the diaphragm and abdominals. The pelvic floor does not independently contract itself but reacts and controls changes in intra-abdominal pressure by working with the diaphragm and abdominals, relaxing briefly on inspiration to allows downward movement of the diaphragm then co contracting with the abdominals during exhalation and coughing allowing upward movement of the diaphragm by increase IAP. Thus, providing active support through constant contraction while passive support of the pelvic occurs through form closure of the sacroiliac joint or SIJ. Force closure of the pelvis refers to interlocking of the joint surfaces, whereas form closure is through compressive forces of the muscles, ligaments, fascia and provides passive stability. Therefore, patients with DRAMS and a weakened linea alba, have poor form closure when performing a curl up task highlighting reduced IAP, reduced trunk mechanics and pelvic instability due to the lack of muscular passive support.
Here at MyoThrive we have an interest in women’s health and will work your women’s health physio or pelvic floor physio for the best outcome 😊
Book an Appoinment