

Pelvic Floor Dysfunction, Menopause & Bladder Health: How It All Connects
The term “pelvic floor” is everywhere now, but many people still aren’t sure what it actually is – or why it can cause so many issues, especially around peri‑menopause and menopause.
At its simplest, the pelvic floor is a group of muscles and connective tissues that sit like a hammock between your tailbone and pubic bone. These muscles:
- Support your bladder, uterus (if present) and bowel
- Help you control urine, bowel movements and wind
- Contribute to sexual function and orgasm
- Work with your deep core to support your spine
When the pelvic floor works well, it contracts and relaxes when it should. When it doesn’t, we call this pelvic floor dysfunction.
Pelvic Floor Dysfunction: More Than Just “Weak Muscles”
Pelvic floor dysfunction isn’t just about weakness. It can involve:
- Underactive (weak) pelvic floor – the muscles don’t contract strongly or for long enough
- Overactive (tight) pelvic floor – the muscles are gripping and can’t easily let go
- Poor coordination – the muscles don’t switch on or off at the right times
Symptoms can overlap between these types, which is why guessing and doing random Kegels can sometimes make things worse.
What can contribute to pelvic floor dysfunction?
Factors include: 
- Pregnancy and childbirth (vaginal or caesarean)
- Chronic coughing (asthma, smoking, chronic lung issues)
- Hormonal changes in peri‑menopause and post‑menopause
- Pelvic pain conditions (e.g. endometriosis, painful periods)
- Prostate surgery/treatment in men
- Obesity
- Chronic constipation and straining
- High‑impact sport or heavy lifting without adequate support
- Stress and habitual “holding” patterns (e.g. always bracing your tummy or glutes)
These influences can lead to weakness, overactivity, or a mix of both.
Signs You Might Have Pelvic Floor Dysfunction
You don’t need to have all of these; even one or two are worth checking out:
- Leaking urine when you cough, sneeze, laugh, jump or run
- Not making it to the toilet in time, strong urgency or loss of bladder control
- Recurrent urinary tract infections (UTIs) or bladder irritation
- Passing wind from the anus or vagina with bending, lifting or exercise
- Heaviness or dragging in the pelvis or lower back (possible prolapse)
- Pain with sex, difficulty with penetration or inability to orgasm
- Reduced sensation in the genital area or during sex
- Difficulty starting the flow of urine, or feeling like you can’t empty fully
- Constipation, straining or pain with bowel movements
Because the same symptom can be caused by either a weak or an overactive pelvic floor, it’s important not to self‑diagnose. A pelvic floor physiotherapist can tell you what’s really going on.
Peri‑Menopause, Menopause, Bladder Infections & the Pelvic Floor
Over the last few years, more research and more menopause‑focused clinicians have been shining a light on how oestrogen, pelvic floor function and bladder health are linked.
Clinicians like Dr Mindy Pelz, Dr Mary Claire Haver, Dr Sara Szal and Dr Lisa Mosconi all highlight the systemic impact of hormonal change in midlife – including on the urinary tract and pelvic tissues.
What happens to the pelvic floor and bladder as oestrogen drops?
In peri‑menopause and post‑menopause:

Photo by Polina Zimmerman on Pexels.com
- The vaginal, urethral and bladder tissues can become thinner and drier
- Blood flow to these tissues decreases
- The natural vaginal microbiome shifts (which can affect infection risk)
- The urethra may not seal as well as it used to
- The pelvic floor muscles can lose bulk and strength
These changes can contribute to:
- Urinary urgency and frequency
- Waking at night to urinate
- Leakage with coughing, sneezing or exercise
- A feeling of incomplete emptying
- Increased risk of recurrent UTIs
- Pelvic floor weakness and/or altered muscle tone
Pelvic floor dysfunction & recurrent UTIs
More recent work has highlighted a few important points:
- A weak pelvic floor can make it harder for the urethra to stay closed, which may increase leakage and irritation around the urinary opening.
- An overactive pelvic floor can make it difficult to fully relax and empty the bladder, which may allow residual urine – and potentially bacteria – to remain.
- Hormonal changes can make the bladder and urethra more vulnerable, so underlying pelvic floor issues become more obvious.
In practice, that means if you’re in peri‑ or post‑menopause and dealing with:
- Recurrent UTIs
- Increased bladder urgency/frequency
- New leakage or pelvic heaviness
it’s worth addressing not only infection treatment and possible vaginal oestrogen (with your GP or specialist), but also your pelvic floor function with a pelvic health physiotherapist.
A Quick Look at Pelvic Floor Anatomy
The main muscles of the pelvic floor belong to the levator ani group:
- Pubococcygeus
- Iliococcygeus
- Coccygeus
They attach from the pubic bone at the front, sweep back to the tailbone, and span side to side like a supportive sling.
These muscles work in partnership with: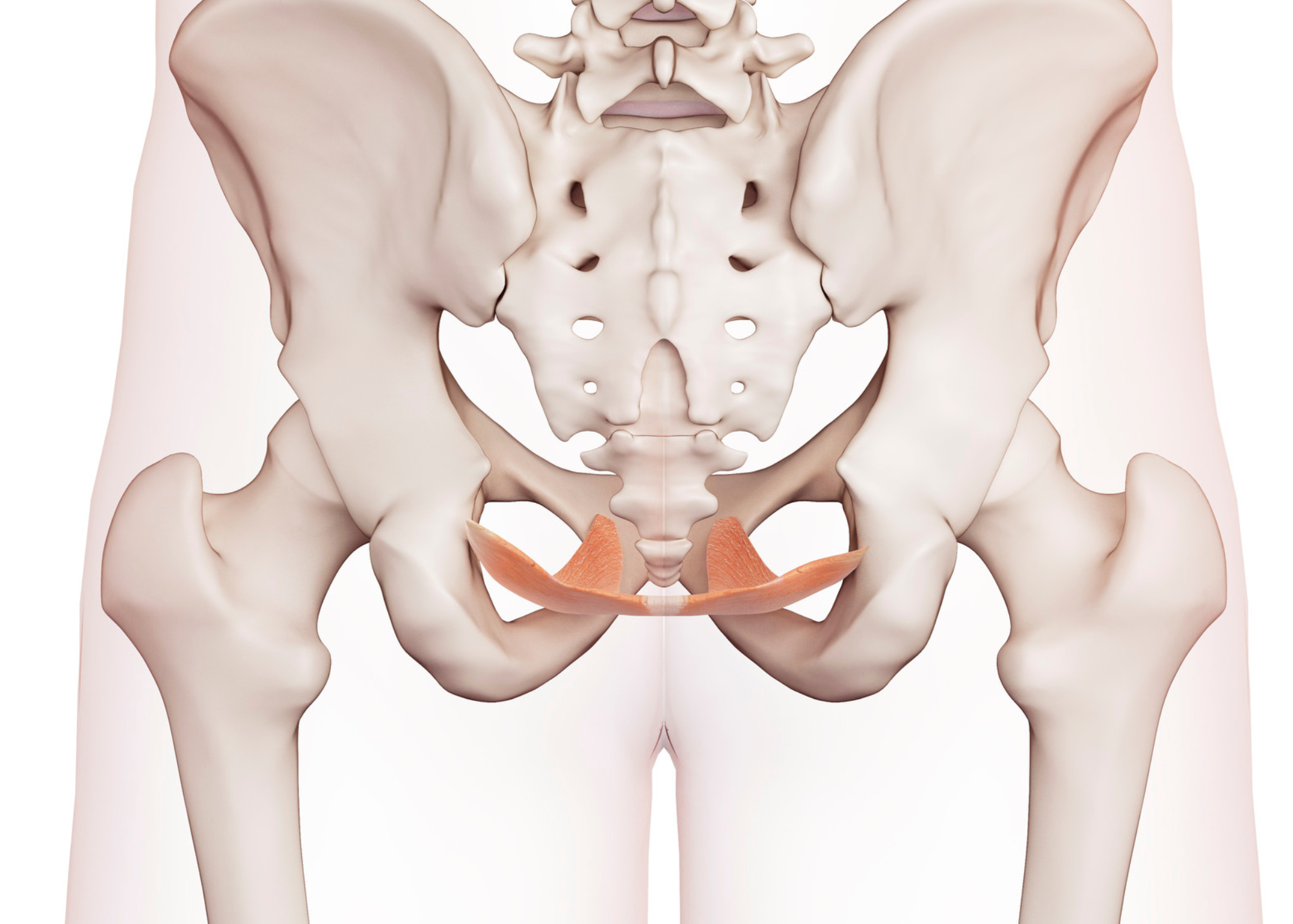
- Deep abdominal muscles (e.g. transversus abdominis)
- Deep back muscles (e.g. multifidus)
- The diaphragm (your main breathing muscle)
Together they:
- Support the pelvic organs
- Help maintain continence
- Stabilise the pelvis and lower back
- Manage pressure in the abdomen when you cough, lift or exercise
How Clinical Pilates Can Help Pelvic Floor Dysfunction
At Myothrive we use Clinical Pilates – Pilates principles combined with clinical assessment – to support people with back pain, pelvic pain and pelvic floor issues.
Clinical Pilates can help both weak and overactive pelvic floors, but the approach is different for each.
For a weak pelvic floor
Clinical Pilates can:
- Teach you how to find and gently activate your pelvic floor
- Integrate pelvic floor support into everyday movements (lifting, rolling, walking, reaching)
- Build endurance, so your pelvic floor supports you throughout the day
- Improve coordination between pelvic floor, deep abdominals, back muscles and breathing
- Progress your strength safely using springs, bands and body‑weight exercises
For an overactive (tight) pelvic floor
When the pelvic floor is overactive, more squeezing is usually not the answer. Clinical Pilates instead focuses on:
- Breathwork and diaphragmatic breathing to promote relaxation
- Gentle mobility for the hips, pelvis and lower back
- “Down‑training”: learning to let go, lengthen and then gently re‑engage the pelvic floor
- Reducing unconscious gripping in the glutes, inner thighs, abdominals and pelvic floor
- Re‑introducing movement in a way that feels safe, to reduce pain‑driven guarding
In both cases, the goal is not just a “strong” pelvic floor, but a responsive, coordinated pelvic floor that can contract, relax and adapt as needed.
Why a Pelvic Floor Specialist Is So Important
Because weak and overactive pelvic floors can look similar from the outside, an assessment is essential before you dive into lots of pelvic floor exercises.
A pelvic floor physiotherapist can:
- Perform an internal exam (with consent) to assess strength, endurance and resting tension
- Identify whether weakness, overactivity, poor coordination or a mix is driving your symptoms
- Check for prolapse, scar tissue and specific pain points
- Work with your GP/gynaecologist/urologist, particularly if you have recurrent UTIs or are in peri‑ or post‑menopause
- Provide a tailored exercise and self‑care plan, and advise whether Clinical Pilates is appropriate right now
If you:
- Have pelvic or bladder pain
- Can’t feel your pelvic floor lifting or relaxing
- Have recurrent bladder infections
- Notice heaviness or bulging vaginally or rectally
- Feel stuck or confused about what exercises are safe
please see a pelvic floor physio.
(For example, we often recommend Jess at 18Physio in Malvern for internal pelvic floor assessment.)
Gentle Pelvic Floor Exercises: Start With Relaxation
If you’ve already been told by a pelvic floor specialist that pelvic floor exercises are suitable for you, these basics can be a starting point. If you’re unsure whether your pelvic floor is weak or overactive, keep the effort light and seek an assessment.
1. Relaxation (for everyone, especially overactive pelvic floors)
- Lie down or sit in a supported position.
- Inhale slowly through your nose, letting your belly and ribs soften and widen.
- As you inhale, imagine your pelvic floor softening and widening – like a flower gently opening or a parachute lowering.
- Exhale and simply rest – avoid any squeezing.
- Repeat 5 times.
This can be used throughout the day, and especially before and after any strengthening work.
2. Gentle warm‑up activation
- Continue the breathing pattern.
- As you exhale, gently lift the pelvic floor as if you’re stopping the flow of urine and holding in wind. Aim for no more than 30–40% effort.
- As you inhale, fully let go and allow the pelvic floor to soften back down.
- Repeat 5 times.
If you feel increased pain, urgency or can’t relax between lifts, stop and book with a pelvic floor physio.
3. Longer holds (for confirmed weakness)
Research in pregnant women suggests 10 contractions of up to 10 seconds, three times daily can improve pelvic floor strength and reduce dysfunction. Many people, however, need to build up gradually.
A gentler progression:
- Exhale and slowly lift the pelvic floor over a count of 3–5 seconds.
- Hold for up to 5 seconds, keeping your breath easy (no jaw clenching or glute squeezing).
- Inhale and completely release the pelvic floor.
- Rest for a breath or two.
- Start with 4–5 repetitions once or twice daily. Add one rep per week if it feels manageable and well‑controlled.
Think of it like starting at the gym: you don’t begin with the heaviest weights. Your pelvic floor needs time to adapt too.
When to Get Extra Help
Reach out to a pelvic floor physio or your GP if you:
- Have pelvic pain or pain with sex
- Have recurrent UTIs or bladder irritation
- Notice new leakage, urgency or pelvic heaviness, especially around peri‑ or post‑menopause
- Can’t feel your pelvic floor engaging or relaxing
- Feel overwhelmed by conflicting advice online
Clinical Pilates at Myothrive can be a valuable part of your pelvic health plan – especially when combined with proper pelvic floor assessment and, when needed, medical or hormonal support.
If you’d like to know whether Clinical Pilates is appropriate for you right now, you can book a free 15‑minute consult via our website: www.myothrive.com.au.
Further Learning & Research
If you’d like to dive deeper into menopause and pelvic health, the following clinicians and areas of research are useful starting points:
- Dr Mary Claire Haver – evidence‑based menopause management, including weight, inflammation and metabolic health (all of which can affect pelvic floor load and tissue quality).
- Dr Sara Szal – pelvic health and women’s health education, with a focus on practical strategies for managing pelvic floor dysfunction and incontinence.